Leaderboard
-
Prozac
Supreme User6Points1,714Posts -
brabus
Supreme User4Points4,712Posts -
Stitch
Supreme User4Points568Posts -
ThreeHoler
Supreme User3Points2,320Posts




Popular Content
Showing content with the highest reputation on 11/25/2020 in all areas
-
4 pointsSource for all past, present, and future data: CDC. I will state if different, but prefer to stick with CDC because that’s likely the most accurate/apolitical data we have. Since you clearly didn’t read everything I wrote, I’ll reiterate that I said multiple times these numbers are nationwide average for under 70, which makes up the vast majority of our population (~90%...technically 87% up to age 64, 2010 census brackets 65+ into one group; so clearly 69 and under accounts for more than 87%). So yes, “disclaimer” clearly stated, and you are being deceptive/attempting to discredit data because it doesn’t fit your opinion, and hoping others haven’t actually read my posts and just assume your misrepresentation of such is accurate. Absolutely none of this is misleading or inaccurate, it is 100% factual straight from the CDC. I can’t help that you don’t like the numbers, but they are quite literally unemotional, apolitical, and as accurate as the CDC is capable of producing. Now, to your age group point: making public policy and systemic level decisions based on 10% of the population is unsound my opinion. Why would you not make decisions based on how it affects the majority (in this specific case, we’re talking data points that represent a MASSIVE majority: ~90%). The 2019 average life expectancy was 78.8, so dying beyond that, regardless of cause, is beating life expectancy. That doesn’t mean their lives weren’t important to others, but unemotionally they have done better than average. Got it, cue bleeding heart; my point is emotional decision making is an awful failure when exercised at state and federal levels (and still usually bad even at a personal level). To make public policy based on 10% of the population who are already above average age, that negatively impacts the rest of the population, is emotional decision making at its worst and terribly short-sighted. Since you’ll probably respond with a demand for how I’d solve it - well, we should look at policy that aims to provide isolation OPTIONS for that age group, while allowing the other 90% access to the things they need to live life (and that includes things that contribute to mental well being). Let the 70+ demographic choose how to proceed - it’s their life and they should make the call, not the government. Maybe you don’t talk to enough 70+ year olds, because all of my family and friend’s families who are in that bracket are pissed and just want to be the ones who decide for themselves. Stop treating them like children who can’t make adult decisions. But what about the hospitals? I agree, that’s an important question to ask/valid data point to take into account when making decisions. As of 14 Nov, COVID hospitalization rate is 228.7 per 100k population. Breaking it down to specifically COVID cases relative to number of those that end in hospitalization - 0.59%. All from the CDC, covering the entire age range. I get it that in city X it is way worse than that, but its disingenuous to yell about that city while ignoring city Y that isn’t overrun at all. We’re talking state/federal level policy here, or at least I am.4 points
-
4 pointsHope for the future; 17 year old girl gets PPL in spring of 2020, goes on to place second in a major STOL competition.4 points
-
3 pointsNewsflash: MyCS is a troll and wasting everyone’s time. Welcome back Shazam and whatever else you called yourself before. Sent from my iPhone using Baseops Network mobile app3 points
-
3 points"Command post". Not "Commander". At least, that's how I read it.3 points
-
2 pointsThat’s like saying you could avoid second hand smoke by never leaving the house. Look, you argue in your previous post that mass shutdowns aren’t really a feasible option. I’m inclined to agree with you. So let’s take seriously the relatively small sacrifices we’re being asked to make. Wearing a mask in public, or even skipping one Thanksgiving with the family is a pretty small price to pay to keep the economy running. Let’s make the mental and physical investments it’s going to take & get through this thing.2 points
-
2 pointsLess than 3000 Americans died in the attacks on Sept 11 and we made some pretty significant policy based on that event. ~60k Americans were killed in the Vietnam war over 10 years and that is widely considered to be a great travesty. Are we really going to say that because COVID-19 only affects the old and/or vulnerable that we should disregard a quarter of a million fatalities? Think about that for a minute. A quarter of a million deaths in less than a year. When is the last time this country dealt with fatalities like that? WWII? The Civil War? What kinds of sacrifices did everyday Americans make then? This idea that people have lived full lives and should thus be discarded is kind of sickening. If a cancer patient gets hit by a bus, guess what? It’s not the cancer that killed them. We don’t make the speed limit 75mph through retirement communities with the attitude that the people there have lived full lives & why should the rest of us be inconvenienced by slowing down? Now, is shutting down the entire economy necessary? Should our kids be denied their education? How much stimulus can a government that’s already in debt afford? Those are all valid questions and there is a pretty wide spectrum of reasonable answers given that this is the first time in modern history that a developed society has had to deal with something like this. Maybe, just maybe though, we could soften the blow a little bit if we were willing to make a few small sacrifices for one another.2 points
-
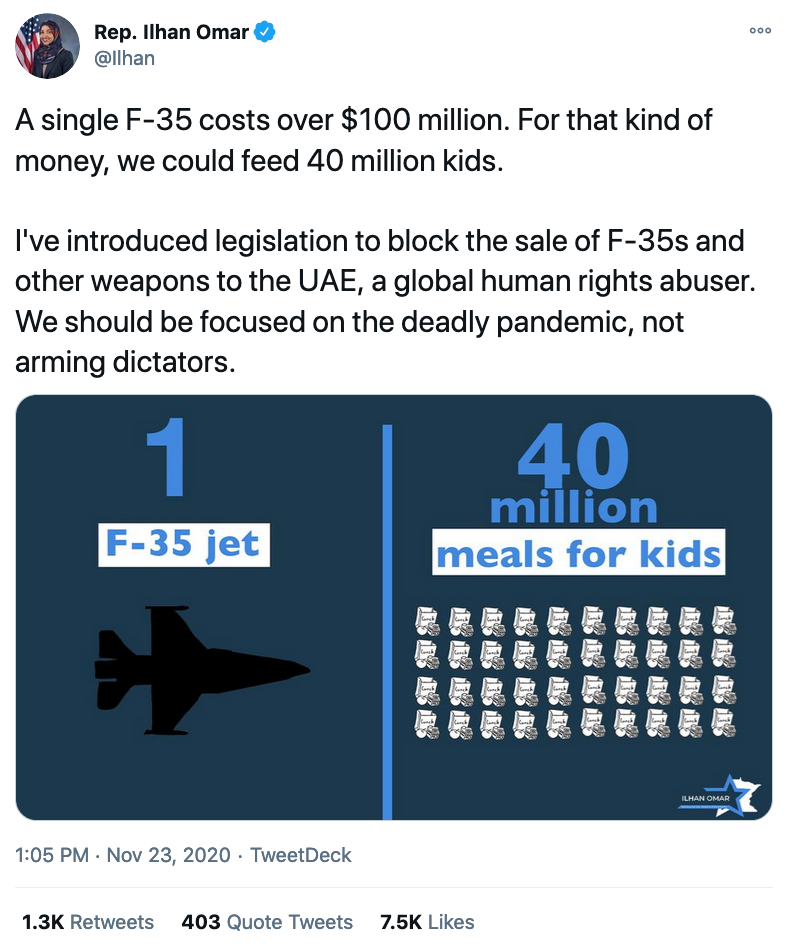
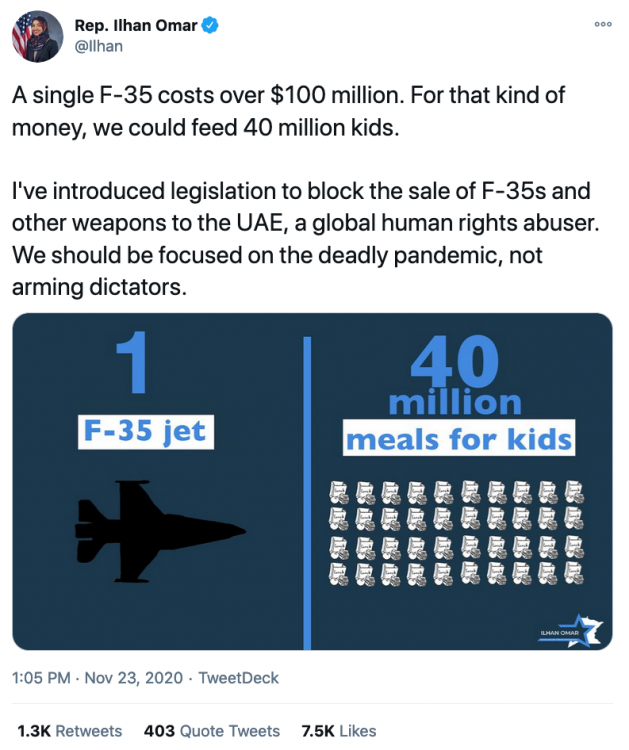
2 points2 points2 pointsYou have to put a disclaimer with your “99.86%” every time you write it or else you are being intentionally deceptive. What you meant to say was a 99.86% survival rate for people up to the age of 40, I assume. Also, let’s see your sources. The problem with this talking point is that it entirely skews the whole problem. Literally everyone has known for months now that young people will be okay. But as soon as you hit 50-59 your case fatality rate hits 0.5-1.0%. 60-69 is 2-4%. The real problem, though, is that 70 year olds have a 5-10% mortality rate and 80 year olds have a 15%+ mortality rate. And you’re ignoring that? This is the actual issue, and you can’t just gloss over the portion of mortality that doesn’t fit your narrative because it’s convenient. Although I have noticed talk radio loves to try. It’s akin to saying “Cancer/heart disease/[insert literally 90% of diseases] isn’t important to study because it largely doesn’t affect young people.” Now if you want to say that you’ve accepted the risk of older people dying - that that is a sacrifice we should make as a society - then at least you’re being genuine. Realistically there obviously has to be balance, but saying this isn’t a disease that’s more fatal than the flu and trying to discredit it with misleading statistics adds nothing to the conversation. Heres an actual source with case fatality rates: https://ourworldindata.org/mortality-risk-covid2 points2 pointsHere you guys go. You now have your very own spot to argue. It’s your spot and yours alone. Have it here so the rest of us can enjoy what baseops is supposed to be about. Lloyd2 points2 pointsThe only way I'd go back to that part of the world is with a fully nuke loaded B-52/B-1/B-2 but I know a couple of guys who enjoy it over there.2 points2 pointsBecause blocking the sale of US exports, manufactured by US moms and dads, feeds kids. UAE would probably be disappointed with their "F-35s", anyway.
 2 points2 pointsFlying at HRT the Navy pogues from Pcola and Whiting would always trash our pattern, sometimes four or five at a time. After the three times being told to extend my base while doing two engine training in order to accommodate a T-34, I cleaned up my Gunship and departed VFR to the west. A few minutes later I checked in with PCola and reported initial Runway 25...it was a fucking bomb burst of white jets trying to get out of the way. After a low approach I requested closed and the tower was fuming (do they have a SOF?) I then requested to go tower to tower at Whiting. They initially cleared me but the tower controller must have called Whiting and told them what I did so they told me they were "saturated and could not accommodate practice patterns." I got called up to the OG/CC's office the next morning and he asked what happened...apparently the Navy wasn't too happy. I told him it was a continuing theme with them dorking up our pattern and how they ruined three consecutive two engine approaches (two engine work was challenging and you had to be low on fuel to get to the training allowed weight so you didn't get a lot of second chances). He laughed and told me to have a great day. I didn't see another T-34 in our pattern for two months.2 points1 pointNo, legit, I want to see where you found that. As far as I can tell the CDC only does pandemic planning estimates, and they haven't published any data on actual age related morbidity. It doesn't really matter, as I don't really care about the numbers that much, as long as everyone is on the same page: it doesn't kill young people under 60 basically at all, and it does kill old people at an unreasonably high rate. Hey bro, I'll give you credit for the majority of the times you did say it. But the last time you didn't when you said it was a 12% positive test rate for a disease that has a 99.86% survival rate. Saying a "99.86% survival rate" vs a "99.86% survival rate for the majority of the population" are two ENTIRELY different things. Standard "words matter," and you presented it in a way that makes the impact of COVID - the deaths of old people - not part of the discussion. Let's pretend we didn't do any decision making based on "10% of the population" (~30 million people). If you didn't do anything and let "herd immunity" make it's way around, about 70-80% of the country would get the virus. So ~22 million old people. Of them, 10%+ would die. 2,000,000+ deaths is incalculable. It's hard to imagine, I'm sure, without being personally affected, but that's almost 10 times the number of US soldiers that died in WW2. It's not "unsound" or "emotional" to consider this. It's a moral imperative to consider loss of life like that, especially when they are your American countrymen drowning to death on a ventilator. With that being said, I think that you're right that policy has to consider the 90% as well. There's multiple compromises that no one seems to talk about. I'm a proponent of a temporary monthly living allowance which would go to those over the age of 67 until a vaccine is created while lifting most restrictions for the rest of the 90%. The purpose would be to help those at risk to isolate and pay for services that would enable them to lower their risk of disease (delivery services, nurses, cleaners, grocery services, etc.) This would likely be on the order of ~$1.5k per month or $18k per year/person (adjusted by income), which would come out to $540b a year for approximately 30M people. This is an expense, obviously, but giving money to people that not only need it but would have to spend it would help the economy AND it would enable the other 90% of the population to continue working. If healthy older folks don't want to quarantine, have at it. They can make the risk call themselves. This is America, after all. This seems like an ethical compromise that would probably be cheaper in the long run than having tons of businesses fail while the economy grinds to a halt. And it's better than just choosing to do nothing at all and accepting needless deaths for the economy. In the meantime, distribute information about how you can protect yourself and allow people to make decisions. Some people will make good decisions, and others will do whatever they want, but that's America. Your infection rate will go up. When you get coronavirus - which you probably will - you should be mandated to quarantine until you aren't infectious. It's two weeks, then you are basically good to go. The vaccine will be produced and distributed in 6-12 months, and we're out of the woods. We helped the old people bunker down while still enabling the 90% to pay their rent. The cost would be increased taxes to pay for it, but it would still be cheaper than the economy grinding to a halt and tons of businesses closing. EDIT: Just looked and we've already spent almost $3T on this, with most of it going to where? You and I got $1200, but that only accounts for <10% of the total stimulus. Tax breaks for big companies and millionaires are ruining/diluting actions the government could take to help. Imagine if the government spent half of $3T on ventilators/medical training/medical supplies and gave the rest to individuals at risk to isolate using their own personal liberty and judgment. Here's a pretty good breakdown on how this spending plan unfairly benefits those that it shouldn't (millionaires and billionaires that don't need assistance) https://www.propublica.org/article/the-cares-act-sent-you-a-1-200-check-but-gave-millionaires-and-billionaires-far-more Classic tax cuts for the rich in a pandemic, thanks trickle down economics/Ronald Reagan.1 point1 pointI would absolutely be in favor of regulating the amount of sugar in our food and designing our communities to encourage walking or cycling vs driving, but that’s a whole other conversation brotha! 😎1 point1 pointThe problem is, it’s not just about mitigating your own risk. Think about all the people you come into contact with in day to day life. Coworkers, store clerks, bank tellers, Uber drivers, delivery people, barbers, dry cleaners, etc., etc. Some of those people will likely come into contact with at risk people. Of course, this is a force of nature. We will not be able to stop the spread entirely. But we can use mitigation strategies, and social distancing, masks, and avoiding large gatherings are all strategies that can be effective and that are really not that much of a strain on your personal liberties given what’s at stake.1 point1 pointGoing IMC in a glider with no ADI. I don’t understand how they’re not dead.1 point1 pointIsn’t that the nature of diseases, generally, that they disproportionately affect the older population? Our advances in medicine in the last hundred years have greatly outpaced evolution’s ability to catch up so that immune response stays strong later in life with the increased life expectancy. We already spend a great deal of our medical effort on keeping people alive longer, so it’s a valid discussion on whether the whole of society should be diminished to protect the segment with the least productive potential.1 point1 pointI mentioned it in the COVID thread but there is a HAF/A1 email circulating that says they are examining VSP options for FY21. No details on career fields or numbers though. FY20 had the second highest retention since 2000 (including the year after 9/11).1 point1 point'Member when there was a 3-4 year campaign against Trump because he supposedly was working with Russians to win the election? This is like the same thing, except its the other side. Just let people complain and be skeptical Enjoy your layover in Motel 6 with the FA 🙂1 point1 pointThe dumb thing about all this is it just boils down to "1) if you're sick, stay home until you're completely (and not just mostly) better." And since there's the complication of being contagious with COVID before the onset of symptoms, "2) if you were in close contact with someone who was sick, stay home for a bit a to see if you get symptoms. If you get symptoms, stay home and contact your doctor." But for a whole host of social and economic reasons, that doesn't happen, especially in the US. We could probably be a lot more open right now if people just followed the two rules I led with, even without masks or social distancing. But we as a society can't (won't?) stay home if we're sick, which puts us where we are now. Right or wrong, people are going to work when they probably shouldn't to get that paycheck, and since healthcare is largely tied to employment here. So there's a strong incentive to go to work sick, and maybe take tylenol to knock down any fever and some cough syrup to suppress coughing. Or some people just don't care because it doesn't affect them since their symptoms are mild, so they see it as a non issue. Which is great and all until they interact with someone who is high risk (like a grocery worker or a waiter/waitress who can't stay home to avoid illness despite being high risk, due to bills or lack of sick leave). Still doesn't really affect the original person who was sick, but could be devastating to a stranger that has to interact with them and can't avoid the interaction. As military flyers, especially as pilots, we benefit from having access to decent healthcare, as well as pretty rigorous medical screening early on that identifies underlying conditions, so our peer group is relatively low risk, outside maybe a spouse or kid with health issues. I guess what I'm getting at is there are people/neighbors/fellow Americans that due to circumstance, can't choose to just avoid the whole COVID thing and hunker down (or have a choice to accept risk or not), and have to go in to work and interact with the public. Do we have a responsibility to protect those people? Or does it just suck to be them, and say they're in our thoughts and prayers? I think at least some semblance of a social safety net (such as unemployment benefits, better sick leave policies/regulations, or access to at least emergency healthcare) is needed, and is similar to an ejection seat; should be a last resort, don't ever want to use it, but glad to know it's there if you need it, and hope that the system is maintained in the event it's needed. What percent of sorties require the use of the seat? Fractions of a percent? Cool, we can defer mx due to parts availability... Hopefully we didn't defer other actions or have outside factors (wx, threats) that drive up the likelihood of needing to use that seat.1 point1 point1.) I didn't quote anyone. However, the provided quote was endemic to German thought. I've worked closely with the German government in a security cooperation position and the provided thought process does not surprise me. 2.) What roof? You mean the collapsed plywood on the mud hut in September of 2001? Yeah that was like that when we got there.1 point1 pointFuck'em, let them takeover more of a role if it's so important to them. GTFO of that shit hole tomorrow!1 point1 pointHahahaha. I've been wanting to post this all day but I haven't gotten to it. You beat me first. This dude claims to be able to change car tires but any person with a modest understanding of automobiles wouldn't be caught dead spending 70K on that piece of burning dumpster tampons. It's one of the worst reviewed SUVs ever. If he wanted to impress us he could have at least made up owning a vehicle people found respectable.1 point0 pointsThe RIF was set in motion when the USG decided to cut FY21 DoD budget in 2019. Then in Summer 2020 we announced we are pulling out (STS) of Germany and sending some folks back to CONUS while starbursting then rest all over Europe. We are also pulling chock on AFG. With the AFG troops coming home, what will they be doing? You factor in COVID, no one is leaving the military. We don't have another war to replace AFG (yet) to keep everyone gainfully employed. Also this: https://www.eenews.net/stories/1063718995 https://federalnewsnetwork.com/defense-main/2020/11/focus-on-military-families-defense-strategy-changes-likely-coming-under-biden-administration/ My bet is on Tammy Duckworth to be the next SecDef.0 points
2 points2 pointsFlying at HRT the Navy pogues from Pcola and Whiting would always trash our pattern, sometimes four or five at a time. After the three times being told to extend my base while doing two engine training in order to accommodate a T-34, I cleaned up my Gunship and departed VFR to the west. A few minutes later I checked in with PCola and reported initial Runway 25...it was a fucking bomb burst of white jets trying to get out of the way. After a low approach I requested closed and the tower was fuming (do they have a SOF?) I then requested to go tower to tower at Whiting. They initially cleared me but the tower controller must have called Whiting and told them what I did so they told me they were "saturated and could not accommodate practice patterns." I got called up to the OG/CC's office the next morning and he asked what happened...apparently the Navy wasn't too happy. I told him it was a continuing theme with them dorking up our pattern and how they ruined three consecutive two engine approaches (two engine work was challenging and you had to be low on fuel to get to the training allowed weight so you didn't get a lot of second chances). He laughed and told me to have a great day. I didn't see another T-34 in our pattern for two months.2 points1 pointNo, legit, I want to see where you found that. As far as I can tell the CDC only does pandemic planning estimates, and they haven't published any data on actual age related morbidity. It doesn't really matter, as I don't really care about the numbers that much, as long as everyone is on the same page: it doesn't kill young people under 60 basically at all, and it does kill old people at an unreasonably high rate. Hey bro, I'll give you credit for the majority of the times you did say it. But the last time you didn't when you said it was a 12% positive test rate for a disease that has a 99.86% survival rate. Saying a "99.86% survival rate" vs a "99.86% survival rate for the majority of the population" are two ENTIRELY different things. Standard "words matter," and you presented it in a way that makes the impact of COVID - the deaths of old people - not part of the discussion. Let's pretend we didn't do any decision making based on "10% of the population" (~30 million people). If you didn't do anything and let "herd immunity" make it's way around, about 70-80% of the country would get the virus. So ~22 million old people. Of them, 10%+ would die. 2,000,000+ deaths is incalculable. It's hard to imagine, I'm sure, without being personally affected, but that's almost 10 times the number of US soldiers that died in WW2. It's not "unsound" or "emotional" to consider this. It's a moral imperative to consider loss of life like that, especially when they are your American countrymen drowning to death on a ventilator. With that being said, I think that you're right that policy has to consider the 90% as well. There's multiple compromises that no one seems to talk about. I'm a proponent of a temporary monthly living allowance which would go to those over the age of 67 until a vaccine is created while lifting most restrictions for the rest of the 90%. The purpose would be to help those at risk to isolate and pay for services that would enable them to lower their risk of disease (delivery services, nurses, cleaners, grocery services, etc.) This would likely be on the order of ~$1.5k per month or $18k per year/person (adjusted by income), which would come out to $540b a year for approximately 30M people. This is an expense, obviously, but giving money to people that not only need it but would have to spend it would help the economy AND it would enable the other 90% of the population to continue working. If healthy older folks don't want to quarantine, have at it. They can make the risk call themselves. This is America, after all. This seems like an ethical compromise that would probably be cheaper in the long run than having tons of businesses fail while the economy grinds to a halt. And it's better than just choosing to do nothing at all and accepting needless deaths for the economy. In the meantime, distribute information about how you can protect yourself and allow people to make decisions. Some people will make good decisions, and others will do whatever they want, but that's America. Your infection rate will go up. When you get coronavirus - which you probably will - you should be mandated to quarantine until you aren't infectious. It's two weeks, then you are basically good to go. The vaccine will be produced and distributed in 6-12 months, and we're out of the woods. We helped the old people bunker down while still enabling the 90% to pay their rent. The cost would be increased taxes to pay for it, but it would still be cheaper than the economy grinding to a halt and tons of businesses closing. EDIT: Just looked and we've already spent almost $3T on this, with most of it going to where? You and I got $1200, but that only accounts for <10% of the total stimulus. Tax breaks for big companies and millionaires are ruining/diluting actions the government could take to help. Imagine if the government spent half of $3T on ventilators/medical training/medical supplies and gave the rest to individuals at risk to isolate using their own personal liberty and judgment. Here's a pretty good breakdown on how this spending plan unfairly benefits those that it shouldn't (millionaires and billionaires that don't need assistance) https://www.propublica.org/article/the-cares-act-sent-you-a-1-200-check-but-gave-millionaires-and-billionaires-far-more Classic tax cuts for the rich in a pandemic, thanks trickle down economics/Ronald Reagan.1 point1 pointI would absolutely be in favor of regulating the amount of sugar in our food and designing our communities to encourage walking or cycling vs driving, but that’s a whole other conversation brotha! 😎1 point1 pointThe problem is, it’s not just about mitigating your own risk. Think about all the people you come into contact with in day to day life. Coworkers, store clerks, bank tellers, Uber drivers, delivery people, barbers, dry cleaners, etc., etc. Some of those people will likely come into contact with at risk people. Of course, this is a force of nature. We will not be able to stop the spread entirely. But we can use mitigation strategies, and social distancing, masks, and avoiding large gatherings are all strategies that can be effective and that are really not that much of a strain on your personal liberties given what’s at stake.1 point1 pointGoing IMC in a glider with no ADI. I don’t understand how they’re not dead.1 point1 pointIsn’t that the nature of diseases, generally, that they disproportionately affect the older population? Our advances in medicine in the last hundred years have greatly outpaced evolution’s ability to catch up so that immune response stays strong later in life with the increased life expectancy. We already spend a great deal of our medical effort on keeping people alive longer, so it’s a valid discussion on whether the whole of society should be diminished to protect the segment with the least productive potential.1 point1 pointI mentioned it in the COVID thread but there is a HAF/A1 email circulating that says they are examining VSP options for FY21. No details on career fields or numbers though. FY20 had the second highest retention since 2000 (including the year after 9/11).1 point1 point'Member when there was a 3-4 year campaign against Trump because he supposedly was working with Russians to win the election? This is like the same thing, except its the other side. Just let people complain and be skeptical Enjoy your layover in Motel 6 with the FA 🙂1 point1 pointThe dumb thing about all this is it just boils down to "1) if you're sick, stay home until you're completely (and not just mostly) better." And since there's the complication of being contagious with COVID before the onset of symptoms, "2) if you were in close contact with someone who was sick, stay home for a bit a to see if you get symptoms. If you get symptoms, stay home and contact your doctor." But for a whole host of social and economic reasons, that doesn't happen, especially in the US. We could probably be a lot more open right now if people just followed the two rules I led with, even without masks or social distancing. But we as a society can't (won't?) stay home if we're sick, which puts us where we are now. Right or wrong, people are going to work when they probably shouldn't to get that paycheck, and since healthcare is largely tied to employment here. So there's a strong incentive to go to work sick, and maybe take tylenol to knock down any fever and some cough syrup to suppress coughing. Or some people just don't care because it doesn't affect them since their symptoms are mild, so they see it as a non issue. Which is great and all until they interact with someone who is high risk (like a grocery worker or a waiter/waitress who can't stay home to avoid illness despite being high risk, due to bills or lack of sick leave). Still doesn't really affect the original person who was sick, but could be devastating to a stranger that has to interact with them and can't avoid the interaction. As military flyers, especially as pilots, we benefit from having access to decent healthcare, as well as pretty rigorous medical screening early on that identifies underlying conditions, so our peer group is relatively low risk, outside maybe a spouse or kid with health issues. I guess what I'm getting at is there are people/neighbors/fellow Americans that due to circumstance, can't choose to just avoid the whole COVID thing and hunker down (or have a choice to accept risk or not), and have to go in to work and interact with the public. Do we have a responsibility to protect those people? Or does it just suck to be them, and say they're in our thoughts and prayers? I think at least some semblance of a social safety net (such as unemployment benefits, better sick leave policies/regulations, or access to at least emergency healthcare) is needed, and is similar to an ejection seat; should be a last resort, don't ever want to use it, but glad to know it's there if you need it, and hope that the system is maintained in the event it's needed. What percent of sorties require the use of the seat? Fractions of a percent? Cool, we can defer mx due to parts availability... Hopefully we didn't defer other actions or have outside factors (wx, threats) that drive up the likelihood of needing to use that seat.1 point1 point1.) I didn't quote anyone. However, the provided quote was endemic to German thought. I've worked closely with the German government in a security cooperation position and the provided thought process does not surprise me. 2.) What roof? You mean the collapsed plywood on the mud hut in September of 2001? Yeah that was like that when we got there.1 point1 pointFuck'em, let them takeover more of a role if it's so important to them. GTFO of that shit hole tomorrow!1 point1 pointHahahaha. I've been wanting to post this all day but I haven't gotten to it. You beat me first. This dude claims to be able to change car tires but any person with a modest understanding of automobiles wouldn't be caught dead spending 70K on that piece of burning dumpster tampons. It's one of the worst reviewed SUVs ever. If he wanted to impress us he could have at least made up owning a vehicle people found respectable.1 point0 pointsThe RIF was set in motion when the USG decided to cut FY21 DoD budget in 2019. Then in Summer 2020 we announced we are pulling out (STS) of Germany and sending some folks back to CONUS while starbursting then rest all over Europe. We are also pulling chock on AFG. With the AFG troops coming home, what will they be doing? You factor in COVID, no one is leaving the military. We don't have another war to replace AFG (yet) to keep everyone gainfully employed. Also this: https://www.eenews.net/stories/1063718995 https://federalnewsnetwork.com/defense-main/2020/11/focus-on-military-families-defense-strategy-changes-likely-coming-under-biden-administration/ My bet is on Tammy Duckworth to be the next SecDef.0 points