otsap
Registered User
-
Joined
-
Last visited
Everything posted by otsap
-
The judge in Doster v. Kendall just this morning certified a class action including all Air Force, Space Force, Guard/Reserve, Cadets, etc, and issued a Temporary Restraining Order prohibiting the AF from taking adverse action against unvaxxed members who filed a Religious Accommodation Request that is either still being processed or was denied. The TRO lasts 14 days, DoD has 7 days to respond and argue against class certification. At that point the judge either accepts DoD's argument, unlikely IMO, or more probably issues a Preliminary Injunction.
-
Any updates from folks about this career field? I've been seeing the PSDMs calling for applications to the crossflow board, but still can't tell anyone what the job looks like (TDY/deployment frequency, M-F or shift work, base locations, etc). Thanks in advance for any knowledge or experience you can pass along.
-
Congrats! You had quite the frustrating saga.
-
Got the call yesterday from my SR - selected. PRF: #6/10, P, IDE complete, IPZ
-
Rule of thumb, when you start a sentence with "If you're wondering,...", and no one asked, strongly consider deleting it. Really, I'm just hoping my sarcasm detector is inop and you weren't trying to sound that douchey. But in the event you were serious, semantics cut both ways. To wit: Brickhistory said "legal opinion," which includes your linked article, law review articles, some op-eds, etc. You are referring to a "judicial opinion," a subset of legal opinions noted for setting precedent. As a slight aside, I took National Security Law during law school from a professor who was the CIA's general counsel during Bush #2 and argued for the legality of Hellfire strikes and the drafted the definition of "unlawful combatant." When asked by another student "how can you support those policies," he said, "that was my job." He never elaborated on his true stance. Just thought that was interesting.
-
An important aspect of the "Nordic model" that I don't often hear about, which is germane to the discussion about the U.S. healthcare system, is the massive disparity in medical technology and advancements. The U.S. accounts for 91% of the entire world's medical advances measured by patented devices, therapies, and procedures, as well as peer-reviewed research. That's the power of the profit-motive, for better or worse. For example, the average cost of bringing to market a generic drug (i.e.,Tylenol knockoff) is $500 million. The average cost of a brand new drug is $2 billion. These accounts for research, development, compliance, FDA protocols, and trials. The prices could be lowered, but there's a deleterious effect on safety in doing so. I'm not arguing one way or the other, just pointing out that with a single-payer, Nordic style system, profit motive is diminished if not removed since that system necessitates price controls. Now we could certainly move to that system, but we have to accept a lower level of progress in medical research breakthroughs. This is an area I research and I haven't seen a way around that trade-off. Maybe we're at a point where that's an acceptable policy; after all, medicine has come a long way and universal coverage could arguably be worth it. On the other hand, the medical breakthrough that enables us to repair a damaged spinal cord and reverse a patient's paralysis, which is maybe 10 years away, will now be about 40-50 years away. That's the trade-off, and it's kind of a crappy one to consider no matter which side you take. Medical research is a little expensive, doing it safely is REALLY expensive. Without a profit motive, those breakthroughs will slow; they just will.
-
Not trying to counter your argument, because I agree with what you're highlighting here, but to make it a true apples-to-apples comparison you also have to consider that on the 15 year loan, once it's paid off, all of that monthly payment ($2100/month) would go into that same retirement account for the remainder of the 30 year time period you're discussing. Given the same assumptions of 6%, contributing $2100/month for the final 15 years of the 30 year time period would equal $610,000. Still less than the $664,000 you accrue doing the 30 yr mortgage, but it's a pretty narrow margin that may swing some people's peace-of-mind value toward the 15 yr.
-
Yes! I never would have caught that. He took over while I was going through OTS -- vaguely remember his change of command.
-
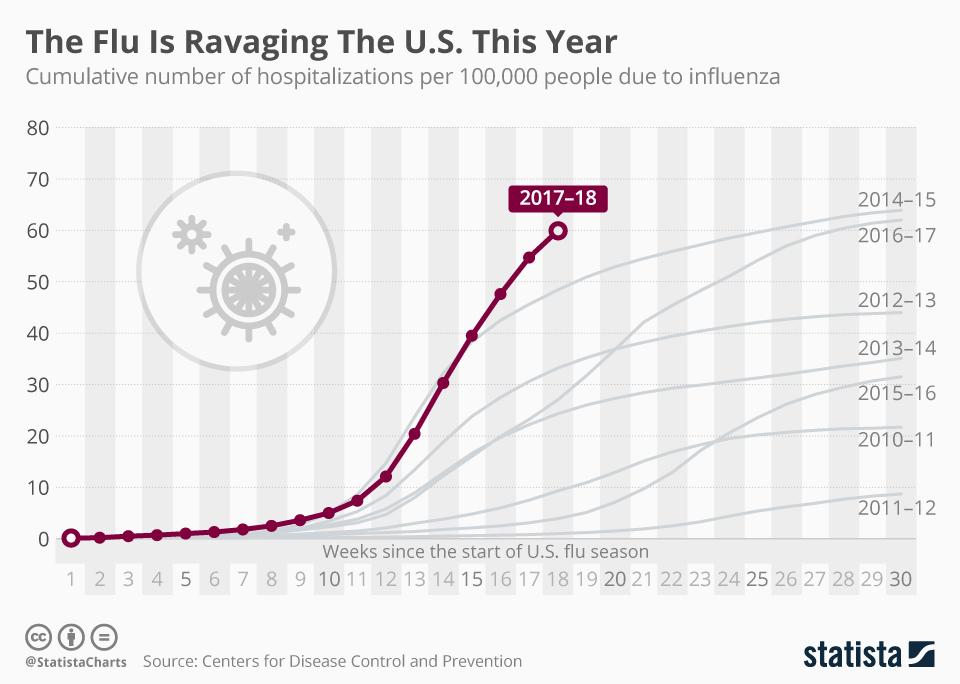
As to the latter part of what you quoted, I don't think I was very clear in my post. I also don't think we'll stay under lockdown -- simply because people won't allow it really -- and I don't think we should. I think my sympathies lie more with those people who lost their jobs and want to work because they need to. I too have noticed that most of the people saying "stay home" are salaried individuals making six figures and up. Granted, that's a function of their leadership role in society (politicians), but it's also coming from doctors, researchers, specialists, and other government employees. "Stay home" is an easy request to make when your paycheck is still coming in; however, the inverse is also true and far more threatening to an individual. With that in mind, I'd also suggest that it's easier to dictate policy based on data sets that are easy to measure, such as number of hospitalizations or deaths. It's far more difficult to dictate policy that results in hospitalizations or deaths when it cannot be as easily linked to the lockdown. But, without a doubt, there will be suicides, domestic abuse, divorces, abandonment, drug and alcohol abuse, et al., attributable to the lockdown due to job loss and economic hardship resulting in increased poverty levels. As to the first comment, I'm not entirely convinced that hospitals are at the breaking point. There may be a few in the hardest hit areas, sure, but that's even true during non-pandemic flu seasons. So it's fair to say that our healthcare system is structurally ill-prepared in the general sense, not specifically because of COVID. I stated earlier that "flattening" the curve is a stupid phrase because the curve looks the same no matter what disease we talk about. Here's the first chart I found showing recent trends: Now, I may be senile, but I don't recall a yearly lockdown that allowed us to "flatten" the above curves for the flu between 2010-2017. This chart shows hospitalization rates for recent flu seasons, and the average is somewhere between 40-50 per 100,000 looking at the left-hand side of that chart. The most recent hospitalization rate for COVID published by the CDC is 20 per 100,000 (source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html. Note that the curve is already flattening at 20, not getting steeper). That's less than half the regular, yearly, non-pandemic, non-media hysteric, flu season hospitalization rate. I know, I'm not a doctor or healthcare specialist. But in the (long) video below, this guy is -- "Professor Johan Giesecke, one of the world’s most senior epidemiologists, advisor to the Swedish Government (he hired Anders Tegnell who is currently directing Swedish strategy), the first Chief Scientist of the European Centre for Disease Prevention and Control, and an advisor to the director general of the WHO:" (highlights include: the novelty of COVID which is a "mild disease" scared people; results will be similar for all countries regardless of mitigation measures; Imperial College paper wasn't published or peer reviewed and shouldn't be used to base policy decisions on; flattening of curve is because most vulnerable die first) * It's just one doctor and I know we could all cherry pick our sources to support our view, but I wanted to show that it's not just my opinion either.
-
I think you're exactly right. What's going to be really irritating is months from now when politicians and talking heads point to the curve and say "Look how it flattened after the lockdowns were put in place." Watch for that, because that argument is going to be made until people accept it as truth, without any discussion of what else may have caused the flattening. You know what other infectious disease curve looks like COVID's and also "flattened out?" EVERY SINGLE ONE EVER. That's how a new/novel disease works. It hurts/kills the most frail and vulnerable early when it initially hits, and then it flattens, because the weakest and most vulnerable are no longer around to be infected. Here's my stab at a logical conclusion that sounds a bit harsh, but seems like reality: A lockdown doesn't make the frail or immunocompromised somehow stronger or less compromised. So the purpose then is to slow the spread until the virus is irradicated or a cure/vaccine is found, which means a lockdown for at least one year by current estimates. But, if we're not prepared for a lockdown until there's a cure or irradication, then the lockdown is again pointless because when lifted, absent a cure or irradication, it will still spread to those who are frail or immunocompromised and they'll end up however they would've ended up anyway.
-
It was in a briefing by my senior rater, but Bigred's source is even better. Also, static closeouts for OPRs. A lot of changes going on.
-
My math may be wrong, but I think it's an 80% chance of promotion for folks that don't have a DP. Using the promotion rate/DP rate of: 90%/50% Say 100 folks are up for promotion for easy math. 50 get DPs and all are promoted. 50 get a P, but to reach a 90% promotion rate, 40 of those with a P would need to get promoted. 40/50=80%....I think. The big change I learned about yesterday is that line numbers will be given based on merit order, rather than date of rank. So the promotion board will rack and stack everyone, and pin-on will occur based on where you end up in that stack. Seems like a good change since you will now know where the board stacked you against your peers. edit: Benny beat me to it
-
On a related topic, here's a link to a website that has mapped out all of the public employees who make more than $95K, with names and job titles: https://www.openthebooks.com/maps/?Map=90001&MapType=Pin As to military pay, it's clearly imbalanced between those who deserve what they're paid, or more, and those whose job doesn't command the pay and benefits they receive. The very few times I've spoken with someone who held the view that military members are paid "too much" or "a ton", I usually ask them, if it's such good pay, why didn't they join? I think once I got the medically unable reason, but the other couple times the person admits "well, when you put it that way..."
-
My last PCS I got orders 7 days before my departure date and TMO said earliest pickup was in 14 days. Our stuff, based on weight, was supposed to take 3 days to pack and 1 day to load according to TMO. Once I got the shipper's name, I called them directly about an earlier pickup. Long story short, they did the the walk-around/survey the next day, and said they could do the whole job 2 days later. It was impressive. 7 dudes showed up, packed and loaded the whole house in 10 hours. As with most things, avoid the bureaucracy and go direct to the source.
-
Quick question for your situation: if you have health insurance through your employer (USAF, airline, etc), did you also carry medical coverage on your auto insurance? Does your state require medical insurance? Did your employer insurance step in at all? Lots of variables to each persons situation, so I'm mostly just curious. I've always refused medical coverages for my auto insurance because we have Tricare and curious now if there's something I'm not considering. Sorry for the goat rope, that blows. I've noticed a dip in USAA's service as well, pretty much across the board. Still better than most banks imo (WF, BoA, etc), but not like it used to be.
-
In what situation, no matter how individualize or niche, would it be preferable to be at a regional instead of major? I only know what I've read in this thread, so pardon the ignorance. But, let's say I don't care about the money so I don't want/need to be a WB CA. Instead, if my primary motivation is the travel benefits, and I would rather fly as seldom as possible, and when I do fly, to fly the shortest legs possible, would it make sense to go regional? I'm thinking doing so would allow me to gain seniority quickly since most people are heading to the majors asap, allowing me to pick lines, flights, schedules, that matched the above desires that much sooner.
-
If you guys read through the Green New Deal, you'd know that the pilot hiring wave is about to hit a brick wall, with furloughs all but inevitable. In an unrelated note, Ocasio-Cortez's campaign contributions were released and her largest donor was the Aircrew Crisis Task Force.
-
Your example is pretty close to a recent reality actually. In July the North Koreans granted clearance to land US Mil cargo in Wonsan (not Pyongyang) for humanitarian purposes (recovery of remains); no natural disaster though. First US Mil in NK since the end of the Korean War. IIRC, the NKs requested commercial air transport and Mattis told them to pound sand, that mil personnel would be brought home on mil aircraft. This was part of Trump's first meeting/negotiation with lil Kim.
-
If you qualify for both GI Bills, you can use a total of 48 months. But, what I've been told is that you have to exhaust the MGIB first, all 36 months of it down to the last day of benefit. Once you do that, then you can utilize 12 months of the Post 9/11 GI Bill. If you switch between them prior to exhausting the MGIB, you will only get 36 total months of benefit, so even if you use 12 months of MGIB, you will then only get 24 months of the Post 9/11. It's due to some caveat/loophole in the Post 9/11 GI Bill, and I believe it carries over to your situation with the transfer as well; meaning as long as no one uses the Post 9/11, you can use all of the MGIB first and get 12 more months on the other. I'd definitely check with the VA before ops checking it. With the much greater value of the Post 9/11 version compared to MGIB, it only seems worth it in unique circumstances.
-
It's comical that anyone would try to assert their financial savvy while simultaneously arguing to buy a $58k vehicle. All the arguments above become moot when compared to a $12k-14k vehicle that is about 4 years old and has around 40k miles on it. What you could do with that extra $44k (!!!) is the real question. Bubububut, reliability! First, 4 year old vehicles with low miles do not lack reliability. Second, even if they did, how many engines/transmissions/exhausts would you have to go through to burn up $44k? Way more than you ever will. Worried about being stuck on the side of the road once or twice during the life of the vehicle? Don't be a baby; it's still not worth $44k.
-
If your son can prove the lie after a not guilty verdict, he might consider suing for defamation. It worked for this Army Colonel who lost his promotion to 1-star after being accused of rape and was discharged. He proved conclusively that he was not even in the state where/when she said it happened, and won over $2 million. She's got a lien against everything she owns now, and probably everything she ever will. https://www.washingtonpost.com/news/true-crime/wp/2017/08/11/jury-orders-blogger-to-pay-8-4-million-to-ex-army-colonel-she-accused-of-rape/?utm_term=.ac0f5735f766
-
Yes please.
-
I want everyone to have access to health care. It sucks to hear stories about people who go bankrupt over medical costs or who suffer permanent or prolonged poor health because of the barriers to care. I want universal health care to work. I especially feel for those with expensive pre-existing conditions. Most people point out the tough financial realities of such a government, or single-payer, program. I don’t disagree that the costs would require a significant increase in taxes from one or more sources. Depending on how much it cost, I wouldn’t necessarily be opposed to it. For example, if taxes went up 4% and everyone was covered, cool, I could live with that. If they go up 15-20% overall, that’s a tough pill to swallow, sts. But my opposition is primarily tied to two other issues that I think are more important long-term. The first is my concern about government creep, a historical near-certainty. Imagine that the government runs health care and sees costs starting to rise; or maybe costs are going down but Congress wants to fund something else and needs to cut its health care costs to fund this other project. Meanwhile, people are pissed because their taxes are going to treat people who smoke, drink, and eat crappy all the time. So, government does what it always does and tries to “fix” this unfairness. Maybe this would result in limiting cigarette purchases, or banning them altogether. Alcohol is unhealthy, so that eventually goes down the same path. Unhealthy foods are taxed more with the idea that these taxes will go to fund the health care system. Over the course of a couple decades, small, almost imperceptible regulations that are passed in the interest of fairness lead to a situation where the government controls (more or less) what you eat, drink, and perhaps even how you act (ie. extreme sports have a higher correlation to injury and long-term health care costs, so even they are restricted). I know hyperbole and the “what-if” game is a poor argument, I’m just trying to suggest that government-run healthcare could EASILY be an invitation to the government to enter the most personal aspects of your life and freedoms. Second, profit-motive is a very hospitable environment to medical advancements. The U.S. is unquestionably the leader in world medical breakthroughs whether that is measured by private and public research expenditures, Nobel prize awards, or published articles and research in medical journals. Today, for a company to bring a generic drug to market it costs between $600-800 million dollars. A brand new drug costs between $2-3 billion dollars. This is the cost of the research, chemistry, FDA wickets, studies, wait times, etc. The reason a company is willing to spend billions is the guarantee of patent protection that allows them to exclusively sell that drug, once it is approved, for a given number of years. (This year, Viagra loses its patent protection FYI) So, Pfizer pays $2 billion for drug X, they have a patent and sell it for whatever they want to recover the costs of development and to make a profit. Government health care necessarily uses price fixing methods to control costs, which removes the profitability of medical research by private companies. If you take away a company’s patent rights or exclusive pricing control, they don’t make money and they don’t research and develop new medicine. (By the way, this isn’t just pharmaceuticals, it’s relevant to medical devices, procedures, techniques, etc) It sucks that medicine might be too expensive for people who need it, or some jackass buys the patent and increases the price 100 fold; I agree they are playing with people’s lives. But I also know that if they didn’t get paid, they wouldn’t have invented or developed the drug in the first place. So I don’t know, I don’t have an answer, just thoughts. But I do think two good places to start would be to look at policies surrounding patent duration and also cutting the cost of FDA approval, thought I know that’s a health and safety concern. Nevertheless…
-
-
You are in desperate need of a topic sentence.